At a well-attended La Trobe University alumni seminar in May 2017, researchers discussed the reality and the hype surrounding mindfulness. They explained the varieties of mindfulness, the clinic research history over the last four decades and the personal advantages of living mindfully. However in the workplace and organisational context, they said that there was insufficient evidence to show benefits from workplace mindfulness in this “emerging area of research”.
At a well-attended La Trobe University alumni seminar in May 2017, researchers discussed the reality and the hype surrounding mindfulness. They explained the varieties of mindfulness, the clinic research history over the last four decades and the personal advantages of living mindfully. However in the workplace and organisational context, they said that there was insufficient evidence to show benefits from workplace mindfulness in this “emerging area of research”.
The seminar was hosted by Latrobe University with three speakers
- Dr Jennifer Arnold-Levy, Director of Making Emotions Work
- Josh Marsden, Manager, Health and Wellbeing La Trobe University and
- Dr Eric Morris, Director of Psychology Clinic, La Trobe University (pictured above.
Many mindfulness advocates have developed programs that they claim can offer substantial benefits to workplaces by increasing productivity and reducing injury and illness, primarily, by changing the behaviours and attitudes of employees. This individual approach is often dropped into a workplace and promoted as an organisational opportunity. But the La Trobe researchers mentioned that this is a very recent perspective.

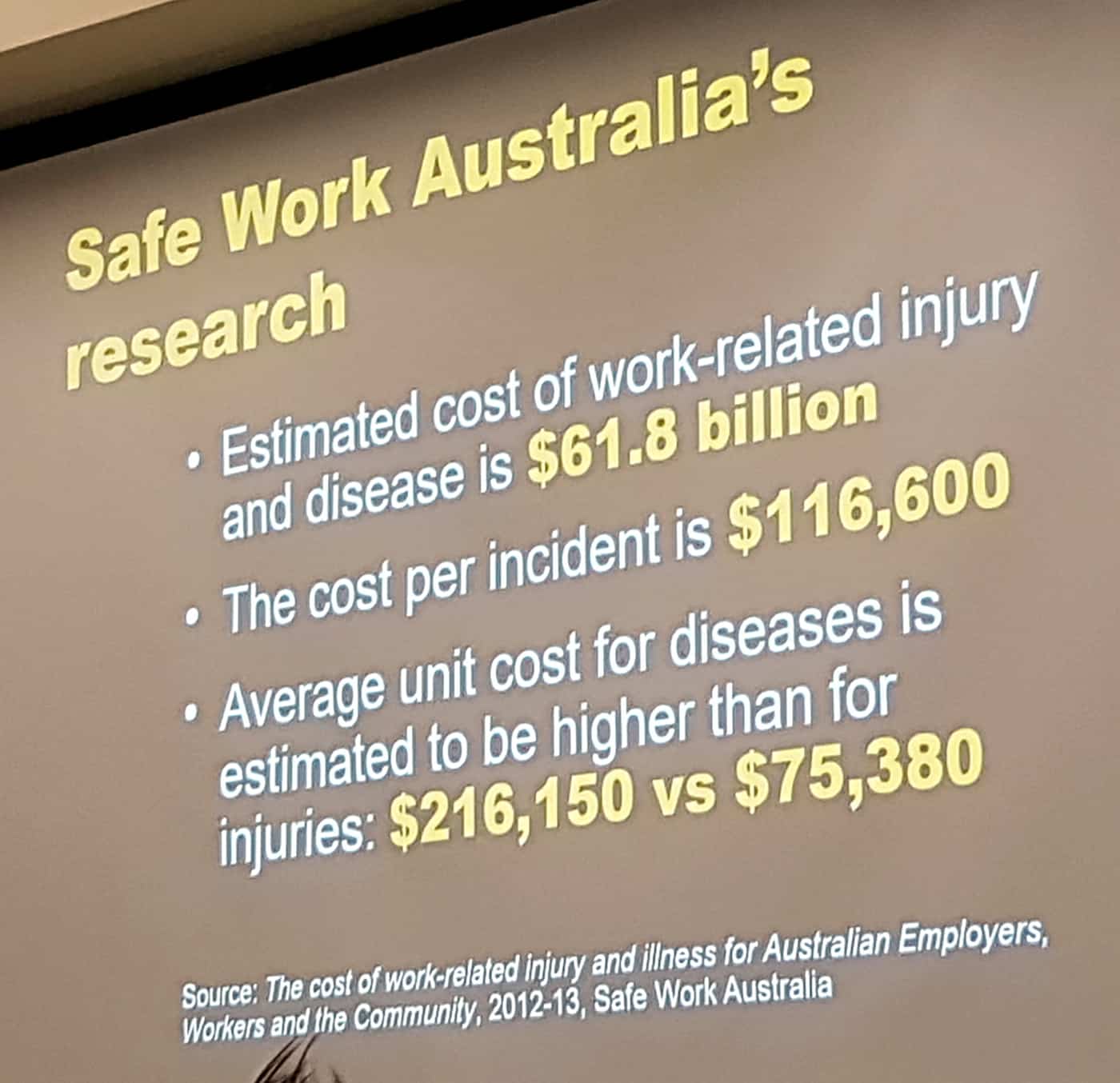
 There has been a lot of discussion recently about occupational health and safety (OHS) data. This article is another because the issue is critical for understanding OHS, for planning for the future and managing productivity.
There has been a lot of discussion recently about occupational health and safety (OHS) data. This article is another because the issue is critical for understanding OHS, for planning for the future and managing productivity.